|
|
|
|
|
|
|
Canine hip
dysplasia (CHD) is a developmental trait primarily affecting medium
and large breed dogs but it is also known |
|
in Cardigan
Welsh Corgis. Many Cardis who are diagnosed with affected hips
however do not seem to suffer a lot from |
|
this defect and
manage to live their life to the max. |
|
|
|
CHD is
characterized by faulty conformation and laxity of the hip joint
that usually affects both hips. It can be detected |
|
radiographically as subluxation of the affected hip. The eccentric
load on the articular surface of the femoral head (ball) |
|
and acetabulum (socket
or cup) leads to erosion of the cartilage, inflammation in the
joint, and debilitating pain. Clinically, |
|
the
osteoarthritis or degenerative joint disease that results from hip
dysplasia is characterized by hind limb lameness, |
|
reduced exercise
tolerance, reluctance to jump, and poor hind limb muscle mass. |
|
|
|
There are
several methods for scoring CHD. In The Netherlands the x-rays are
rated by a panel of three expert evaluators |
|
assigned for
this task by the Dutch Kennelclub, this department is known as GGW
(Health, Behaviour and Wellbeing). |
|
Cardis can be
evaluated from the age of 12 months. In the Netherlands we get an
evaluation based on FCI regulations. |
|
Because of this it
should be possible to compare the scores between the different
countries. Today we still see different |
|
scores in our breed in
certain FCI countries, it raises the question whether the hips of
these dogs are of less quality or if |
|
there is a different method of
scoring within the FCI countries. |
|
|
|
Then there is
the Orthopedic Foundation for Animals that scores hips. Many
Cardigan hips have been evaluated by the |
|
OFA and many
results can be found in the OFA’s database. |
|
|
|
The
phenotypic
evaluation of hips done by the Orthopedic Foundation for Animals
falls into seven different categories. |
|
Those categories
are Normal (Excellent,
Good,
Fair),
Borderline,
and Dysplastic (Mild,
Moderate,
Severe).
Once each of |
|
the radiologists
classifies the hip into one of the 7 phenotypes above, the final hip
grade is decided by a consensus |
|
of the 3 independent
outside evaluations. Examples would be: |
|
|
|
Two
radiologists reported
Excellent,
one
Good—the
final grade would be
Excellent |
|
|
|
One
radiologist reported
Excellent, one
Good, one Fair—the final grade
would be
Good |
|
|
|
One
radiologist reported
Fair,
two
radiologists reported
Mild—the
final grade would be
Mild |
|
|
|
The hip grades of
Excellent, Good and Fair are within normal limits and are given OFA
numbers. This information is |
|
accepted by AKC on dogs with
permanent identification and is in the public domain. Radiographs of
Borderline, Mild, |
|
Moderate and Severely dysplastic
hip grades are reviewed by the OFA radiologist and a radiographic
report is |
|
generated documenting the abnormal
radiographic findings.
Unless
the owner has chosen the open database, |
|
dysplastic hip grades are
not in the public
domain.
|
|
|
|
|
|
|
|
Excellent:
this classification is assigned for superior conformation in
comparison to other animals of the same age and |
|
breed. There
is a deep seated ball (femoral head) which fits tightly into a
well-formed socket (acetabulum) with minimal |
|
joint space. There
is almost complete coverage of the socket over the ball. |
|
|
|
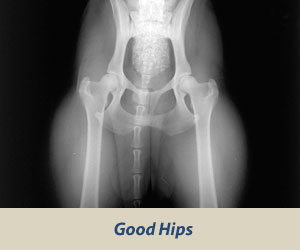
Good:
slightly less than superior but a well-formed congruent hip joint is
visualized. The ball fits well into the socket and |
|
good coverage is
present. |
|
|
|
|
|
|
|
Fair:
Assigned where minor irregularities in the hip joint exist. The hip
joint is wider than a good hip phenotype. This is |
|
due to the ball
slightly slipping out of the socket causing a minor degree of joint
incongruency. There may also be slight |
|
inward deviation of
the weight-bearing surface of the socket (dorsal acetabular rim)
causing the socket to appear slightly |
|
shallow. This can be a
normal finding in some breeds however, such as the Chinese Shar Pei,
Chow Chow, and Poodle. |
|
|
|
Borderline:
there is no clear cut consensus between the radiologists to place
the hip into a given category of normal or |
|
dysplastic.
There is usually more incongruency present than what occurs in the
minor amount found in a fair but there are |
|
no arthritic
changes present that definitively diagnose the hip joint being
dysplastic. There also may be a bony projection |
|
present on any of the
areas of the hip anatomy illustrated above that can not accurately
be assessed as being an |
|
abnormal arthritic change or as
a normal anatomic variant for that individual dog. To increase the
accuracy of a correct |
|
diagnosis, it is recommended
to repeat the radiographs at a later date (usually 6 months). This
allows the radiologist to |
|
compare the initial film with the
most recent film over a given time period and assess for progressive
arthritic changes |
|
that would be expected if the dog
was truly dysplastic. Most dogs with this grade (over 50%) show no
change in hip |
|
conformation over time and receive a
normal hip rating; usually a fair hip phenotype. |
|
|
|
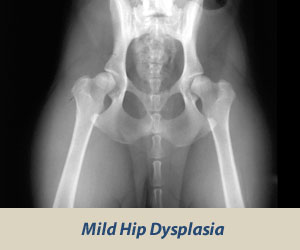
Mild Hip
Dysplasia: there is
significant subluxation present where the ball is partially out of
the socket causing an |
|
incongruent increased
joint space. The socket is usually shallow only partially covering
the ball. There are usually no |
|
arthritic changes present with
this classification and if the dog is young (24 to 30 months of age),
there is an option to |
|
resubmit an radiograph when the dog
is older so it can be reevaluated a second time. Most dogs will
remain dysplastic |
|
showing progression of the disease
with early arthritic changes. Since HD is a chronic, progressive
disease, the older the |
|
dog, the
more accurate the diagnosis of
HD (or lack of HD). |
|
|
|
|
|
|
|
Moderate
Hip Dysplasia: there is
significant subluxation present where the ball is barely seated into
a shallow socket |
|
causing joint
incongruency. There are secondary arthritic bone changes usually
along the femoral neck and head (termed |
|
remodeling),
acetabular rim changes (termed osteophytes or bone spurs) and
various degrees of trabecular bone pattern |
|
changes
called sclerosis. Once arthritis is reported, there is only
continued progression of arthritis over time. |
|
|
|
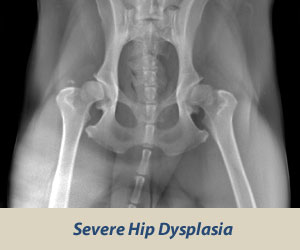
Severe Hip
Dysplasia: assigned
where radiographic evidence of marked dysplasia exists. There is
significant |
|
subluxation present where
the ball is partly or completely out of a shallow socket. Like
moderate HD, there are also large |
|
amounts of secondary
arthritic bone changes along the femoral neck and head, acetabular
rim changes and large |
|
amounts of abnormal bone
pattern changes. |
|
|
|
Here is a
table that shows the different scoring methods. |
|
OFA |
FCI (European) |
BVA
(UK/Australia) |
SV
(Germany) |
|
Excellent |
A-1 |
0-4 (no > 3/hip) |
Normal |
|
Good |
A-2 |
5-10 (no > 6/hip) |
Normal |
|
Fair |
B-1 |
11-18 |
Normal |
|
Borderline |
B-2 |
19-25 |
Fast Normal |
|
Mild |
C |
26-35 |
Noch Zugelassen |
|
Moderate |
D |
36-50 |
Mittlere |
|
Severe |
E |
51-106 |
Schwere |
|
|
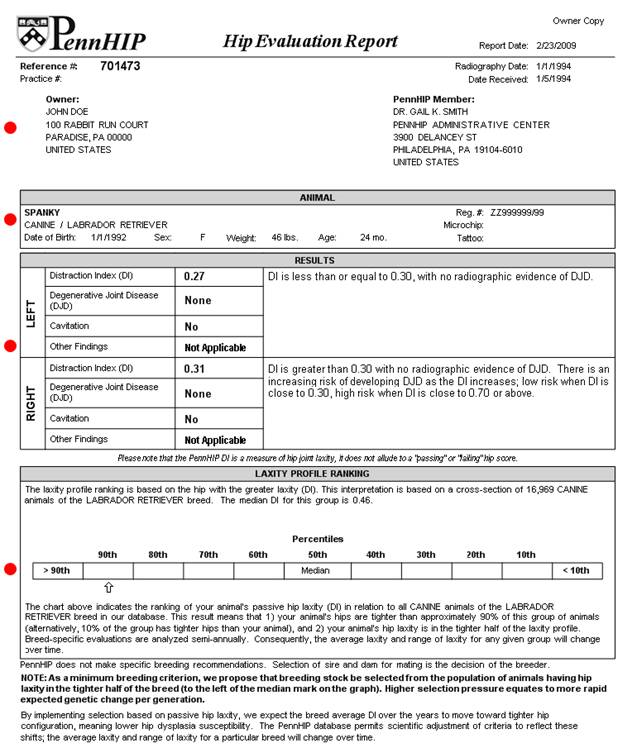
Then there is
the PennHIP method. To go short:
The PennHIP method is
a novel way to assess, measure and interpret |
|
hip
loint laxity.
It consists of three separate radiographs: the
distraction view,
the compression
view
and the |
|
hip-extended
view.
The
distraction view and compression view are used to obtain accurate
and precise measurements |
|
of joint laxity
and congruity. |
|
The
hip-extended view is used to obtain supplementary information
regarding the existence of osteoarthritis |
|
(OA) of the hip
joint. (The hip-extended view is the conventional radiographic view
used to evaluate the integrity of the |
|
canine hip joint.) The
PennHIP technique is said to be more accurate than the current
standard, and it has been shown |
|
to
be a better predictor for the
onset of OA. |
|
|
|
The
radiographs pictured here are of the
same dog,
yet the hip joint laxties in each view look very different. Notice
that |
|
the
hips in
the distraction view appear to be much looser than they do in the
hip-extended view. |
|
|
|
Distraction View |
Compression View |
Hip-Extended View |
|
 |
 |
 |
|
The obvious contrast in joint
laxity between the distraction and hip-extended
views demonstrates |
|
the fundamental difference
between the two radiographs.
The looser the joint on the
distraction |
|
view, the greater is the chance
that the hip will develop OA.
The hip-extended view tends to |
|
mask true hip joint laxity
because the joint capsule is
wound up
into a tightened orientation when |
|
the hips are extended. This
explains why measurable joint laxity on the
distraction view is always |
|
greater than the measurable
laxity from the hip-extended view. In fact,
distraction laxity is up to 11 |
|
times greater depending on the
breed of dog under study. |
|
The compression view is used to
determine the "goodness of fit" of the femoral
heads into the |
|
acetabula. In a hip with OA, the
remodeling that occurs in the acetabulum and/or
the femoral head, |
|
will often result in an
ill-fitting "ball" and "socket". |
|
|
|
|
|
To
summarize, PennHIP method: |
|
|
|
* |
Obtains OA readings from the standard hip-extended view |
|
* |
Obtains hip joint congruity readings from the compression view |
|
* |
Obtains quantitative measurements of hip joint laxity from the
distraction view |
|
|
|
 |
|
|
|
CHD in dogs
is an inherited, polygenic trait in which mutations in
several genes called quantitative trait loci (QTLs) |
|
contribute to its
clinical expression. Many dogs with normal hips on radiographs carry
at least a modicum of the trait- |
|
causing mutations but not all
that are necessary to cause physical expression of the trait. CHD is
a quantitative or |
|
complex trait that is expressed as a
continuum from imperceptible to severe forms. This continuum of
trait expression is |
|
due to environmental influences (such as
plane of nutrition and exercise, as well as other unknown factors)
which |
|
interact with the genetic constitution to affect the
degree to which the trait is manifested. |
|
|
|
CHD has a
heritability between 0.20-0.7. This means that between 20 and 70% of
the physical appearance of the hips |
|
of each dog in a
pedigree can be attributed to its genetic relationships within the
pedigree. |
|
|
|
It will take
a concerted effort to rid breeds of the genetic mutations that cause
CHD or conversely, to introduce |
|
protective alleles at
the loci that cause good hips. Selective breeding based on current
radiographic methods can |
|
reduce the frequency of CHD in a
population. Breeding two dysplastic dogs can yield a 75%
incidence of hip |
|
dysplasia in offspring, while mating two
unaffected dogs can yield a 25% incidence of the disease.
Selective |
|
breeding using normal dogs from normal
parents and grandparents, as well as progeny testing, should
decrease the |
|
incidence of CHD. |
|
|
|
Until there
is a genetic test for CHD, so we can detect genetically susceptible
dogs, the best indication of a dog's |
|
genetic makeup is
where it came from (its' parents and grandparents), what it produces
(its' offspring), and the |
|
phenotype of its' siblings or
half sibs. Dogs with normal hip radiographs that carry some of the
mutations that cause |
|
CHD but perhaps not the major
ones, when bred to a mate that also carries some of the mutations
for CHD, may |
|
produce affected offspring. |
|
|
|
To test
whether a dog carries some of the mutations (even if the dog has
OFA-good hips), it should be bred to sires |
|
or dams with good
hips and the proportion of affected offspring recorded (progeny
testing). As many as 15-20 |
|
offspring should be produced to
be reasonably sure that the parents do not carry important mutations.
This is an |
|
unreasonable burden for dog breeders to
bear. Breeders should attempt to breed dogs with the best hips in |
|
their colony as well as to dogs with the other
optimal breed characteristics and temperament. |
|
|
|
At the
Cornell University Hospital for Animals in New York they have been
searching for the genes that contribute |
|
to hip dysplasia.
When an owner comes to this hospital for hip radiographs, they are
asked to donate a small |
|
sample of blood from their dog for
DNA isolation. This DNA and the hip radiograph measurements are then
used |
|
later to discover and confirm the mutations
that contribute to hip dysplasia. Once they know which genes and
|
|
biochemical pathways lead to good and poor hip conformation,
they can develop novel treatments which can be |
|
applied at an early
age. |
|
|